
Introduction
Telemedicine-delivered medication for opioid use disorder (TMOUD) became more prevalent during the COVID-19 pandemic. This was a positive development that had potential to increase access to evidence-based treatment for a population heavily affected by the opioid crisis. Despite the increase in the use of TMOUD, there were no established service- and process-focused models to guide implementation.
This study aimed to develop a process- and service-focused implementation model in collaboration with key stakeholders and bring together peer-reviewed literature, practice-based knowledge, and expert opinions.
Methods
Step 1: Define scope and objectives
This model focused on developing and improving processes (e.g. workflows, roles, infrastructure) to support TMOUD implementation, rather than setting clinical standards or analysing barriers. A participatory approach was prioritised, drawing on clinical expertise and professional values. The model was context-sensitive, collective, and aligned with implementation theories like Normalization Process Theory, distinguishing TMOUD from standard MOUD, identifying key stakeholders, and outlining necessary processes and appraisal methods.
Step 2: Gather supporting evidence
Due to limited TMOUD-specific implementation evidence, we conducted inclusive, iterative scoping reviews and collected expert case studies via addiction professional networks (e.g. ISAM, CSAM) to inform model development.
Step 3: Engage stakeholders
We identified stakeholders via Scotland’s 31 ADPs, national advocacy groups, research networks, and professional bodies. As TMOUD had little presence locally, we initiated a web-based event featuring expert presenters from multiple countries. Participants could engage via live chat and indicate interest in future involvement.
Step 4: Draft the implementation model
The initial draft drew on policy reviews, expert input, transcripts from the engagement event, and evidence from TMOUD implementation literature and case studies.
Step 5: Consult stakeholders
The draft was shared via PDF and a web-based platform for asynchronous feedback. Some participants requested emailed copies due to access or privacy concerns. All feedback was reviewed and discussed in a final roundtable with key decision-makers.
Step 6: Finalise model
The revised draft was updated with ongoing literature findings and stakeholder input, resulting in the final TMOUD implementation model based on combined evidence, expert insight, and participatory engagement.
Results
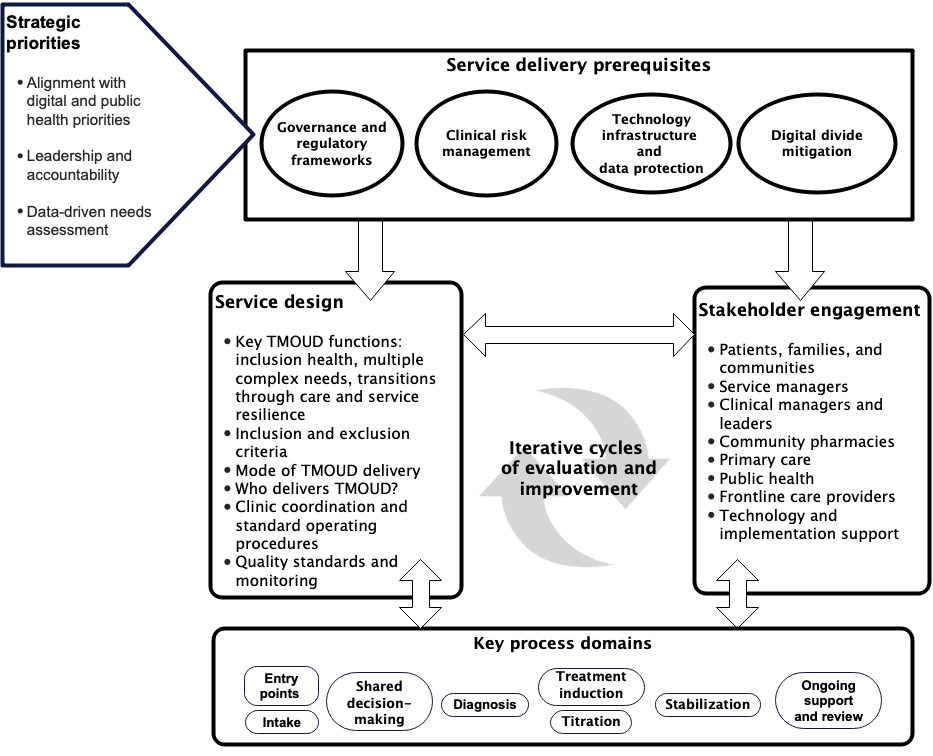
The final specification for the TMOUD implementation model incorporated key strategic priorities, service delivery prerequisites, service design elements, stakeholder identification and engagement, key process domains, and iterative cycles of evaluation and improvement.
Through stakeholder engagement and key informant consultation, we produced a process- and service-focused TMOUD implementation model. The model is modifiable to different contexts and settings while also in keeping with the current evidence base and national and international standards of high-quality opioid use disorder care.
Source: doi:10.2196/47186
Outputs
Tay Wee Teck J, Gittins R, Zlatkute G, Oteo A, Galea-Singer S, Baldacchino A. (2023) Developing a theoretically informed implementation model for telemedicine-delivered medication for opioid use disorder: A qualitative study with key informants. JMIR Ment Health 2023;10:e47186. DOI: 10.2196/471863
Tay Wee Teck J, Butner J, Baldacchino A. (2023) Understanding the use of telemedicine across different opioid use disorder treatment models: A scoping review. Journal of Telemedicine and Telecare 2023. DOI: 10.1177/1357633X231195607
Tay Wee Teck J, Zlatkute G, Perez A … Galea-Singer, S, Baldacchino A. (2023) Key implementation factors in telemedicine- delivered medications for opioid use disorder: a scoping review informed by normalisation process theory. The Lancet Psychiatry 2023; 10: 50–64. DOI: 10.1016/S2215-0366(22)00374-1